Overview  The Achilles tendon connects the muscles in the back of your lower leg to your heel bone. It allows you to move your foot down (?step on the gas? motion). This movement is essential for walking, running, and jumping. A sudden strong contraction of the lower leg (such as when playing sports) can partially tear or rupture the Achilles tendon. This injury is more likely if there is prior injury or inflammation of that tendon from prior stress. You may feel a pop or snap, or like you have been kicked. An Achilles tendon tear will cause local swelling and pain and difficulty in walking. A complete Achilles rupture is usually treated with surgery to attach the torn ends of the tendon. This is followed by 6-8 weeks in a walking cast, boot, or splint. Nonsurgical treatment is an option, but it will take longer to heal and the risk of repeat rupture is greater. With either type of treatment, you will need a physical therapy program to strengthen your Achilles tendon. It will take 4-6 months to return to your former level of activity. Causes An Achilles tendon injury might be caused by several factors. Overuse. Stepping up your level of physical activity too quickly. Wearing high heels, which increases the stress on the tendon. Problems with the feet, an Achilles tendon injury can result from flat feet, also known as fallen arches or overpronation. In this condition, the impact of a step causes the arch of your foot to collapse, stretching the muscles and tendons. Muscles or tendons in the leg that are too tight. Achilles tendon injuries are common in people who participate in the following sports. Running. Gymnastics. Dance. Football. Baseball. Softball. Basketball. Tennis. Volleyball. You are more likely to tear an Achilles tendon when you start moving suddenly. For instance, a sprinter might get one at the start of a race. The abrupt tensing of the muscle can be too much for the tendon to handle. Men older than age 30 are particularly prone to Achilles tendon injuries. Symptoms Patients who suffer an acute rupture of the Achilles tendon often report hearing a "pop" or "snap." Patients usually have severe pain the back of the lower leg near the heel. This may or may not be accompanied by swelling. Additionally, because the function of the Achilles tendon is to enable plantarflexion (bending the foot downward), patients often have difficulty walking or standing up on their toes. Diagnosis Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis. Non Surgical Treatment Treatment of the initial injury is with use of ice, elevation, and immobilization. If suspected you should contact your podiatrist or physician. Further treatment with continued immobilization, pain medication, or anti-inflammatory medications may be advised. If casted the foot is usually placed in a plantarflexed position to decrease the stretch on the tendon. As healing progresses the cast is changed to a more dorsiflexed position at the ankle. The casting processes can be up to 8 weeks or more.
The Achilles tendon connects the muscles in the back of your lower leg to your heel bone. It allows you to move your foot down (?step on the gas? motion). This movement is essential for walking, running, and jumping. A sudden strong contraction of the lower leg (such as when playing sports) can partially tear or rupture the Achilles tendon. This injury is more likely if there is prior injury or inflammation of that tendon from prior stress. You may feel a pop or snap, or like you have been kicked. An Achilles tendon tear will cause local swelling and pain and difficulty in walking. A complete Achilles rupture is usually treated with surgery to attach the torn ends of the tendon. This is followed by 6-8 weeks in a walking cast, boot, or splint. Nonsurgical treatment is an option, but it will take longer to heal and the risk of repeat rupture is greater. With either type of treatment, you will need a physical therapy program to strengthen your Achilles tendon. It will take 4-6 months to return to your former level of activity. Causes An Achilles tendon injury might be caused by several factors. Overuse. Stepping up your level of physical activity too quickly. Wearing high heels, which increases the stress on the tendon. Problems with the feet, an Achilles tendon injury can result from flat feet, also known as fallen arches or overpronation. In this condition, the impact of a step causes the arch of your foot to collapse, stretching the muscles and tendons. Muscles or tendons in the leg that are too tight. Achilles tendon injuries are common in people who participate in the following sports. Running. Gymnastics. Dance. Football. Baseball. Softball. Basketball. Tennis. Volleyball. You are more likely to tear an Achilles tendon when you start moving suddenly. For instance, a sprinter might get one at the start of a race. The abrupt tensing of the muscle can be too much for the tendon to handle. Men older than age 30 are particularly prone to Achilles tendon injuries. Symptoms Patients who suffer an acute rupture of the Achilles tendon often report hearing a "pop" or "snap." Patients usually have severe pain the back of the lower leg near the heel. This may or may not be accompanied by swelling. Additionally, because the function of the Achilles tendon is to enable plantarflexion (bending the foot downward), patients often have difficulty walking or standing up on their toes. Diagnosis Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis. Non Surgical Treatment Treatment of the initial injury is with use of ice, elevation, and immobilization. If suspected you should contact your podiatrist or physician. Further treatment with continued immobilization, pain medication, or anti-inflammatory medications may be advised. If casted the foot is usually placed in a plantarflexed position to decrease the stretch on the tendon. As healing progresses the cast is changed to a more dorsiflexed position at the ankle. The casting processes can be up to 8 weeks or more. 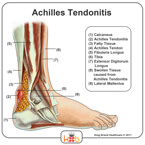 Surgical Treatment Referral to a surgeon for open or percutaneous repair of the tendon is often necessary, followed by an immobilisation period. Functional bracing and early mobilisation are becoming more widely used postoperatively. There is no definitive protocol for this and it may differ, depending on the surgeon. Operative treatment has a reduced chance of re-rupture compared with conservative treatment (3.5% versus 12.6%) and a higher percentage of patients returning to the same level of sporting activity (57% versus 29%). The patient's desired functional outcome and comorbidities that affect healing will be factors in the decision to operate. Prevention To help prevent an Achilles tendon injury, it is a good practice to perform stretching and warm-up exercises before any participating in any activities. Gradually increase the intensity and length of time of activity. Muscle conditioning may help to strengthen the muscles in the body.
Surgical Treatment Referral to a surgeon for open or percutaneous repair of the tendon is often necessary, followed by an immobilisation period. Functional bracing and early mobilisation are becoming more widely used postoperatively. There is no definitive protocol for this and it may differ, depending on the surgeon. Operative treatment has a reduced chance of re-rupture compared with conservative treatment (3.5% versus 12.6%) and a higher percentage of patients returning to the same level of sporting activity (57% versus 29%). The patient's desired functional outcome and comorbidities that affect healing will be factors in the decision to operate. Prevention To help prevent an Achilles tendon injury, it is a good practice to perform stretching and warm-up exercises before any participating in any activities. Gradually increase the intensity and length of time of activity. Muscle conditioning may help to strengthen the muscles in the body.
The Achilles tendon connects the muscles in the back of your lower leg to your heel bone. It allows you to move your foot down (?step on the gas? motion). This movement is essential for walking, running, and jumping. A sudden strong contraction of the lower leg (such as when playing sports) can partially tear or rupture the Achilles tendon. This injury is more likely if there is prior injury or inflammation of that tendon from prior stress. You may feel a pop or snap, or like you have been kicked. An Achilles tendon tear will cause local swelling and pain and difficulty in walking. A complete Achilles rupture is usually treated with surgery to attach the torn ends of the tendon. This is followed by 6-8 weeks in a walking cast, boot, or splint. Nonsurgical treatment is an option, but it will take longer to heal and the risk of repeat rupture is greater. With either type of treatment, you will need a physical therapy program to strengthen your Achilles tendon. It will take 4-6 months to return to your former level of activity. Causes An Achilles tendon injury might be caused by several factors. Overuse. Stepping up your level of physical activity too quickly. Wearing high heels, which increases the stress on the tendon. Problems with the feet, an Achilles tendon injury can result from flat feet, also known as fallen arches or overpronation. In this condition, the impact of a step causes the arch of your foot to collapse, stretching the muscles and tendons. Muscles or tendons in the leg that are too tight. Achilles tendon injuries are common in people who participate in the following sports. Running. Gymnastics. Dance. Football. Baseball. Softball. Basketball. Tennis. Volleyball. You are more likely to tear an Achilles tendon when you start moving suddenly. For instance, a sprinter might get one at the start of a race. The abrupt tensing of the muscle can be too much for the tendon to handle. Men older than age 30 are particularly prone to Achilles tendon injuries. Symptoms Patients who suffer an acute rupture of the Achilles tendon often report hearing a "pop" or "snap." Patients usually have severe pain the back of the lower leg near the heel. This may or may not be accompanied by swelling. Additionally, because the function of the Achilles tendon is to enable plantarflexion (bending the foot downward), patients often have difficulty walking or standing up on their toes. Diagnosis Diagnosis is made by clinical history; typically people say it feels like being kicked or shot behind the ankle. Upon examination a gap may be felt just above the heel unless swelling has filled the gap and the Simmonds' test (aka Thompson test) will be positive; squeezing the calf muscles of the affected side while the patient lies prone, face down, with his feet hanging loose results in no movement (no passive plantarflexion) of the foot, while movement is expected with an intact Achilles tendon and should be observable upon manipulation of the uninvolved calf. Walking will usually be severely impaired, as the patient will be unable to step off the ground using the injured leg. The patient will also be unable to stand up on the toes of that leg, and pointing the foot downward (plantarflexion) will be impaired. Pain may be severe, and swelling is common. Sometimes an ultrasound scan may be required to clarify or confirm the diagnosis. MRI can also be used to confirm the diagnosis. Non Surgical Treatment Treatment of the initial injury is with use of ice, elevation, and immobilization. If suspected you should contact your podiatrist or physician. Further treatment with continued immobilization, pain medication, or anti-inflammatory medications may be advised. If casted the foot is usually placed in a plantarflexed position to decrease the stretch on the tendon. As healing progresses the cast is changed to a more dorsiflexed position at the ankle. The casting processes can be up to 8 weeks or more. Surgical Treatment Referral to a surgeon for open or percutaneous repair of the tendon is often necessary, followed by an immobilisation period. Functional bracing and early mobilisation are becoming more widely used postoperatively. There is no definitive protocol for this and it may differ, depending on the surgeon. Operative treatment has a reduced chance of re-rupture compared with conservative treatment (3.5% versus 12.6%) and a higher percentage of patients returning to the same level of sporting activity (57% versus 29%). The patient's desired functional outcome and comorbidities that affect healing will be factors in the decision to operate. Prevention To help prevent an Achilles tendon injury, it is a good practice to perform stretching and warm-up exercises before any participating in any activities. Gradually increase the intensity and length of time of activity. Muscle conditioning may help to strengthen the muscles in the body.
